



🩸 RED BLOOD JOURNAL
REPORT #1832 – PART I
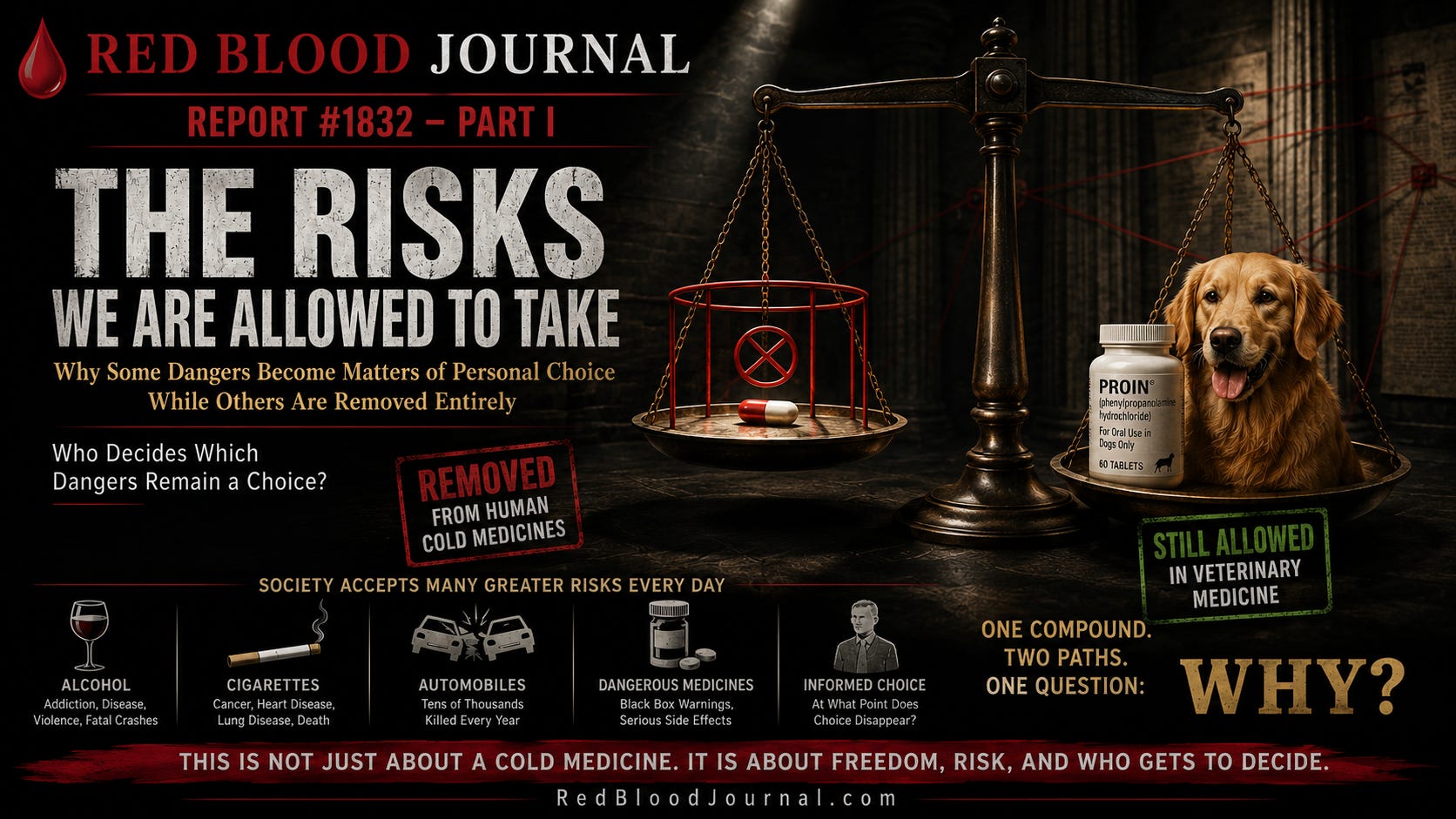
THE RISKS WE ARE ALLOWED TO TAKE
Why Some Dangers Become Matters of Personal Choice While Others Are Removed Entirely
Executive Summary
Every society decides which risks its people may voluntarily accept.
Some dangers remain matters of personal choice.
Others become matters of regulation.
A smaller number disappear entirely.
Those decisions are rarely explained by danger alone.
Automobiles kill tens of thousands of people every year.
Alcohol contributes to disease, addiction, violence, and fatal accidents.
Cigarettes remain one of the leading preventable causes of death worldwide.
Prescription medications carrying black-box warnings continue to be prescribed under physician supervision because regulators conclude that, for some patients, the potential benefits outweigh the risks.
Society generally manages these dangers through education, warning labels, licensing, professional oversight, and informed consent.
Yet not every product receives the same opportunity.
Some medicines are removed completely.
Others are preserved through increasingly sophisticated systems of supervision.
This report examines one such case.
For decades, millions of Americans relied upon a cold medicine known as Comtrex.
Many who used it remember it as unusually effective.
Then one of its principal ingredients—phenylpropanolamine (PPA)—disappeared from human over-the-counter medicine.
The official explanation was safety.
The evidence deserved serious consideration.
Hemorrhagic stroke is a catastrophic medical event.
No responsible discussion should minimize that reality.
But another question remains.
Was complete elimination the only possible regulatory response?
Or were other paths available that were never seriously explored?
This investigation does not argue that PPA was harmless.
It does not suggest that old formulations should simply return to pharmacy shelves.
Instead, it asks a broader question:
How does society decide which risks adults may knowingly accept and which choices disappear entirely?
The answer extends far beyond one cold medicine.
It reaches into medicine, regulation, economics, institutional incentives, and the philosophy of informed consent.
This is where the investigation begins.
Chapter 1
The Medicine People Still Remember
Most medicines disappear quietly.
Few are remembered decades after they vanish.
Comtrex is different.
Ask enough people who used the original formulation, and a remarkably consistent memory emerges.
It was the medicine they reached for when a cold was beginning.
The congestion would start.
Breathing became difficult.
The nose continuously ran.
The throat became irritated.
Body aches appeared.
Energy disappeared.
Within a short period after taking the medicine according to its directions, many users remember becoming functional again.
The cold itself had not disappeared.
Viruses cannot be erased by a multi-symptom cold medicine.
But something important had changed.
They could breathe.
They could sleep.
They could think clearly.
They could continue working.
For someone attempting to care for a family, finish a workday, or simply rest through the night, that difference mattered.
Effectiveness in medicine is often misunderstood.
A treatment does not need to cure a disease to provide meaningful benefit.
Reducing suffering is itself a legitimate medical objective.
Helping a patient sleep while their immune system recovers has value.
Reducing fever has value.
Allowing hydration by opening swollen nasal passages has value.
Helping a parent care for children while sick has value.
Medicine is not only about eliminating disease.
It is also about reducing human suffering.
That distinction matters because many people who remember the original Comtrex are not claiming it cured infections.
They are saying something much simpler.
It worked.
That collective memory does not establish scientific proof.
Neither should it be dismissed.
Patient experience has often been the beginning—not the end—of medical investigation.
Chapter 2
What Was Inside the Original Comtrex?
Over the years, Comtrex appeared in multiple formulations.
Ingredients changed as regulations evolved and manufacturers updated products.
One of the most recognizable combinations included medicines intended to treat several symptoms simultaneously.
The formula commonly contained:
• Acetaminophen — to reduce pain and fever.
• Chlorpheniramine — an antihistamine intended to reduce nasal drainage and sneezing.
• Dextromethorphan — to suppress persistent coughing.
• Phenylpropanolamine (PPA) — a sympathomimetic decongestant intended to reduce swelling inside the nasal passages and improve airflow.
Each ingredient served a different purpose.
Together they attempted to relieve the collection of symptoms people associate with the common cold.
The formula did not eliminate viruses.
It did not shorten every illness.
It attempted something equally practical:
To help people continue living while their bodies recovered.
Millions relied upon medicines built on exactly that philosophy.
Chapter 3
The Disappearance
Most consumers never witnessed what happened.
One year their medicine existed.
A few years later it did not.
Many assumed it had simply been replaced by something newer.
Others believed manufacturers had improved the formula.
Few realized that one ingredient had effectively vanished from human over-the-counter medicine in the United States.
That ingredient was phenylpropanolamine, commonly abbreviated PPA.
The public explanation appeared straightforward.
Research had raised concerns regarding hemorrhagic stroke.
Regulators concluded that the risks justified removing PPA from human over-the-counter products.
For many people, the story ended there.
But every investigation should begin with a simple habit:
Whenever a conclusion appears obvious, examine how that conclusion was reached.
What evidence existed?
How strong was it?
Did it apply equally to every form of use?
Were alternative regulatory options considered?
Could risk have been managed differently?
Or did complete removal become the only acceptable outcome before every alternative had been explored?
Those questions are not signs of rejecting science.
They are examples of scientific thinking.
Science advances by asking difficult questions—not by refusing to ask them.
Chapter 4
Understanding Risk
Every medicine carries risk.
Aspirin can produce gastrointestinal bleeding.
Acetaminophen can cause severe liver injury when taken in excessive amounts.
Antibiotics may trigger life-threatening allergic reactions.
General anesthesia carries measurable risks despite modern safety improvements.
The existence of danger does not automatically eliminate a treatment from medical practice.
Instead, physicians and regulators constantly compare two realities:
Potential benefit.
Potential harm.
That comparison rarely produces absolute certainty.
It produces judgment.
Some medicines remain available despite substantial risks because the expected benefit justifies carefully managed use.
Others remain available only by prescription.
Others require laboratory monitoring.
Others require specialized physicians.
Others require signed informed consent.
Medicine has never been free of danger.
It has always been the art of managing danger responsibly.
That principle makes the PPA story particularly interesting.
Because the central question is not whether danger existed.
The central question is whether complete elimination represented the only responsible method of managing that danger.
Chapter 5
The Yale Hemorrhagic Stroke Project
The turning point arrived with a major investigation known as the Yale Hemorrhagic Stroke Project.
Researchers examined whether use of phenylpropanolamine was associated with hemorrhagic stroke.
Their work deserved serious attention.
Hemorrhagic stroke is uncommon compared with ischemic stroke, but when it occurs the consequences can be devastating.
The study identified an increased association between certain uses of PPA and hemorrhagic stroke.
Importantly, however, the strongest association did not arise uniformly across every use of the medication.
One of the clearest signals involved women using PPA-containing appetite suppressants, particularly during first use.
The findings involving cough-and-cold medicines were more complex.
That distinction is significant.
Recognizing differences among formulations, doses, durations of use, and patient populations is a normal part of scientific evaluation.
Regulators ultimately concluded that the remaining uncertainty justified removal from human over-the-counter medicines.
Reasonable people may agree or disagree with that conclusion.
What deserves careful examination is not whether the study existed.
It unquestionably did.
The question is whether every potential regulatory response between unrestricted over-the-counter sales and complete elimination received equal consideration.
That question leads directly to the next chapter of this investigation.
End of Part I
Continued in Report #1832 – Part II, where the investigation examines regulatory alternatives, informed consent, physician judgment, veterinary phenylpropanolamine, and the broader question of how societies choose which risks remain matters of personal choice and which are removed entirely.
🩸 The Philosophy of Risk and the Disappearance of PPA
Jul 17, 2026
This report from the Red Blood Journal explores the philosophical and regulatory tension between individual liberty and public safety through the lens of a discontinued cold medication. The text specifically examines phenylpropanolamine (PPA), a former key ingredient in products like Comtrex that was removed from shelves due to its association with hemorrhagic strokes. While acknowledging the medical risks identified by the Yale Hemorrhagic Stroke Project, the author questions why this specific substance was banned entirely while other dangerous items like alcohol and tobacco remain matters of personal choice. By contrasting the perceived effectiveness of original medicine formulas with the finality of government regulation, the source challenges how society determines which risks adults should be allowed to manage through informed consent. Ultimately, the investigation asks if total elimination was the only responsible path or if alternative oversight could have preserved access to a highly valued treatment.
